What is the evidence for surgical reconstruction of a PCL injury?
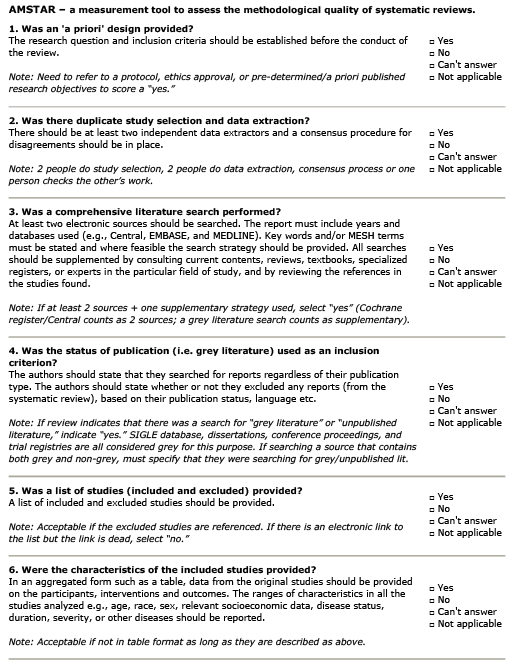
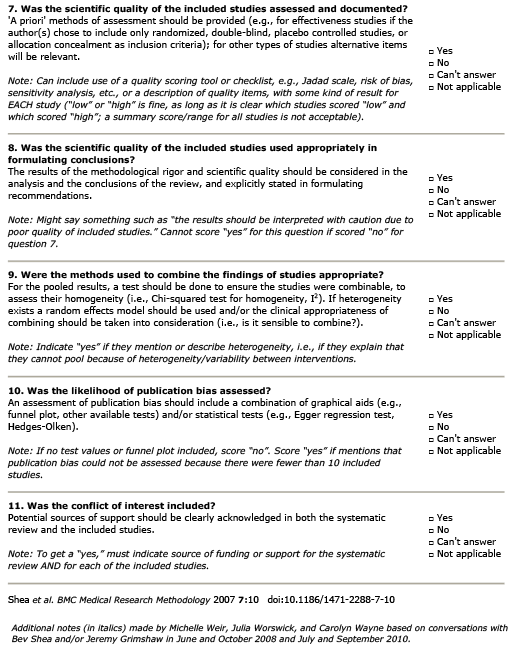
AMSTAR Rating
Summary
Patient Population:
In the 21 studies of isolated reconstruction: Sample sizes ranged from 11-55. Reported mean ages ranged from 26-39. In the 10 studies of combined reconstruction: Sample sizes ranged from 11 – 41. Reported mean ages (years) ranged from 25-33.
Intervention:
Reconstruction techniques included: anteromedial (AM), anterolateral (AL) transtibial tunnel drilling technique in single bundle arthroscopic PCL reconstruction using hamstring tendon autograft and preservation of the PCL remnant, 4-strand hamstring tendon or 7-strand hamstring tendon autografts; single bundle or double bundle, transtibial or tibial inlay techniques; 1-incision or 2-incision arthroscopic PCL reconstruction; and autograft or allograft (with variations in graft source – quadriceps vs. achilles or tibialis anterior).
Comparison:
There were 21 studies of isolated PCL reconstructions identified. Only one of these 21 studies was a prospective, comparative (Level II) study. Additionally, 10 studies describing combined PCL reconstructions were identified for inclusion. All 10 were retrospective case series. Mean reported length of follow-up in the 21 studies of isolated reconstruction ranged from 24 – 109 months. In the 10 studies of combined PCL reconstruction: mean follow-up ranged from 24-66 months when reported. However, some studies did not report a mean and may have followed some participants for longer periods.
Outcome:
- Graft Failure: There were 6 isolated and 2 combine studies that reported graft failure rates. Reported failure rates ranged from 2.3% (comparing 4-strand hamstring tendon autograft with 7-strand hamstring tendon autograft; only 1 failure in the 4-strand group) to 30% (a study comparing tibial versus transtibial inlay techniques; 2/7 graft failures in the tibial inlay group and 4/13 in the transtibial group). Overall, review authors reported graft failure rate across all studies of 11.6%.
- Range of Motion: 16/21 and 9/10 of the isolated and combined reconstruction publications, respectively, provided estimates of knee range of motion. None of the retrospective comparative studies reported significant between group differences in range of motion. Higher rates of manipulation under anesthesia (MUA) were reported in studies of combined rather than isolated reconstruction.
- Activity Level: A single comparative study reported a significant negative outcome over time (single bundle PCL reconstruction) and a single study reported a significant improvement over time (7-strand vs. 4-strand autograft). However, the majority of comparative studies noted no significant between group differences in terms of return to activity (isolated PCL reconstructions).
- Knee Laxity: In a single study, there was a significant difference reported in posterior knee laxity between groups receiving 4-strand hamstring tendon autograft reconstruction and those receiving 7-strand hamstring tendon autograft reconstruction. However, the review authors note that there were no other significant between group comparisons reported in terms of posterior knee laxity.