What is the evidence for radiofrequency ablation for facet joint and sacroiliac joint related lower back pain?
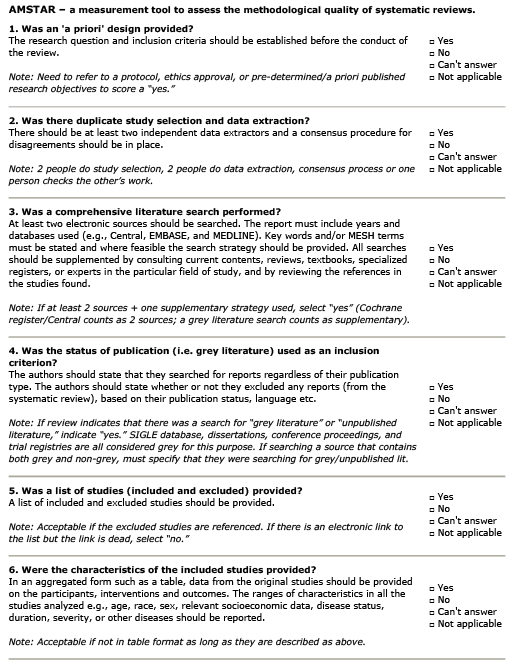
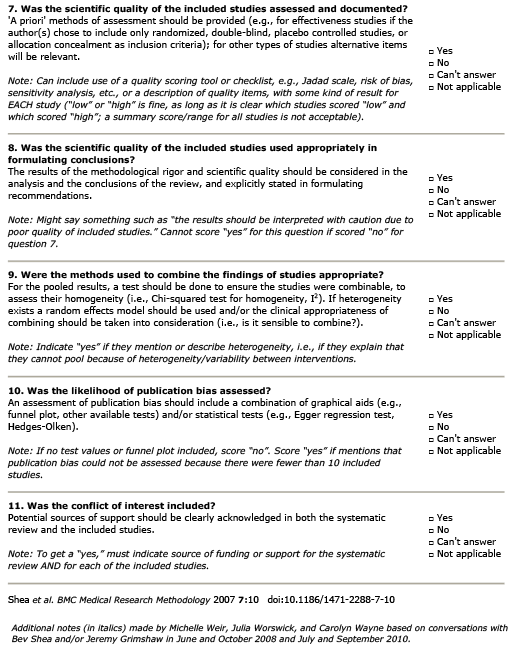
AMSTAR Rating
Summary
Patient Population:
13 randomized controlled trials (RCTs) were included in this study with a total of 747 participants. As one RCT did not report sex and age as a demographic, ~50.2% of participants were male, and mean age of participants was ~54.2. Eight studies focused on patients with lumbar pain, two on cervical pain, and three on sacroiliac joint pain.
Intervention:
Study experimental groups used radiofrequency ablation (RFA) as their intervention. Eight RCTs used pulsed radiofrequency (PRF), while five trials used continuous radiofrequency (CRF). Follow-up durations between studies span from six to 12 months. Temperature of RFA ranged between 40°C and 90°C, and timing of the procedure ranged from 90 seconds to 360 seconds.
Comparison:
All studies compared their RFA intervention groups to corticosteroid injections (CSI). The studies incorporated a combination of corticosteroids and local anesthetics for these comparison groups. Methylprednisolone was used in six trials, typically in dosages ranging from 20 mg to 40 mg and often combined with varying amounts of bupivacaine. Betamethasone, used in three trials, had dosages ranging from 3 mg to 12 mg, while dexamethasone, used in two trials, was consistently dosed at 10 mg. Additionally, triamcinolone was used at 10 mg. These steroids were frequently combined with local anesthetics such as bupivacaine or lidocaine to enhance their effectiveness.
Outcome:
Pain intensity was assessed through the visual analogue scale (VAS) or numerical rating scale (NRS) at three, six, and 12 month follow-up periods. Functional disability was measured with the Oswestry Disability Index (ODI) at a three-month follow-up.
- CSI groups reported statistically significantly higher pain intensity compared to RFA groups at three months (SMD=0.92; 95% CI: 0.19 to 1.65), and six months (SMD=1.53; 95% CI: 0.66 to 2.40).
- Subgroup analysis based on joint type demonstrated that CSI correlated with higher pain intensity compared to RFA in patients with sacroiliac (SMD=1.25; 95% CI: 0.39 to 2.11) and lumbar (SMD=1.33; 95% CI: 0.09 to 2.57) pain at three months. The same was found at six months for sacroiliac (SMD=1.62; 95% CI: 0.79 to 2.45) and lumbar (SMD=1.94; 95% CI: 0.92 to 2.97) pain.
- CSI treatment was found to have negative and not statistically significant results compared to RFA in patients with cervical pain at three months (SMD=-0.40; 95% CI: -0.90 to 0.10) and six months (SMD=-024; 95% CI: -0.72 to 0.26).
- Pain levels were comparable and not statistically significant between RFA and CSI groups at 12 months (SMD=1.47; 95% CI: -0.03 to 2.97). At 12 months, pain intensity scores in patients with sacroiliac (SMD-0.10; 95% CI: -0.52 to 0.72) and lumbar (SMD=1.82; 95% CI: -0.03 to 3.66) pain were also comparable.
- Patients that received CSI had statistically significantly higher ODI scores compared to RFA (SMD=1.28; 95% CI: 0.20 to 2.35) at three months. CSI was also correlated with significantly higher ODI scores than RFA specifically with sacroiliac (SMD=075; 95% CI: 0.01 to 1.50) and lumbar (SMD=1.41; 95% CI: 0.08 to 2.73) pain.
Guideline Recommendations
| Source | Recommendation |
|---|---|
| North American Spine Society (2020) | GRADE B (Moderate) support for RFA for Facet; GRADE C (weak) support for SI |
| American Society of Interventional Pain Physicians (2020) | LEVEL II (Moderate) support for Cervical/Lumbar, LEVEL III (Weak) support for Thoracic |
| National Institute for Health and Care Excellence (NICE) (2020) | Recommend for MOD/SEVERE Facet pain resistant to Non-surgical treatment |
Outcomes Assessed
- Benefit
- Harm
- Inconclusive
Pain
Lumbar facet (3 and 6 months)
SI joint (3 and 6 months)
Cervical (3, 6 and 12 months)
Lumbar/SI (12 months)
Function
Lumbar (3 and 6 months)
SI Joint (3 and 6 months)
Potential Side Effects
Minor burns
Moderate Pain (during procedure)
Neuropathy
Relevant Clinical Info
Hashemi M, Hashemian M, Mohajerani SA, Sharifi G. Effect of pulsed radiofrequency in treatment of facet-joint origin back pain in patients with degenerative spondylolisthesis. Eur Spine J. 2014 Sep;23(9):1927-32. doi: 10.1007/s00586-014-3412-x. Epub 2014 Jul 6. PMID: 24997616.
Hashemi et al. (2014) conducted a RCT to evaluate the efficacy of RFA compared to CSI for lumbar spondylolisthesis. A total of 80 participants (Male=57, Female=23, average age of 64.1 years) with at least six months of lower back pain and grade I spondylolisthesis were split equally into RFA and CSI groups. Under fluoroscopic guidance, the PFA groups received PRF at 42°C in 120 second intervals (two shots of 45V/s) and the CSI group received 1ml (40 mg) triamcinolone and 0.5ml bupivacaine 0.5%. Researchers used the NRS to measure pain outcomes and found that mean NRS scores for low back pain reduced significantly from 7.4±1.1 at pre-treatment to 2.4±1.9 at six months (p=0.035) in the RFA group. While at six weeks, there was no significant difference between PFA and CSI group NRS scores, RFA significantly reduced NRS at 12 weeks (p=0.012) and six months (p=0.02) compared to CSI. The ODI was also used to assess functional outcomes, finding that ODI scores dropped from 75.6±14.3% at pre-treatment to 19.3±9.5% at six months (p=0.001) in RFA patients. While at six weeks there was no significant difference between RFA and CSI ODI scores (p=0.31), researchers found that there was a significant difference between the groups at 12 weeks (p=0.022) and six months (p=0.03). These results suggest that with time (after 12 weeks), pain decreases, and function increases more after RFA intervention compared to CSI.
Participant Information
of participants
were Male
The sample size was 747
Mean age of 54.2 years.
There were 13 studies used.