What is the evidence for suprascapular nerve blocks in patients with chronic shoulder pain for pain reduction and functional improvement?
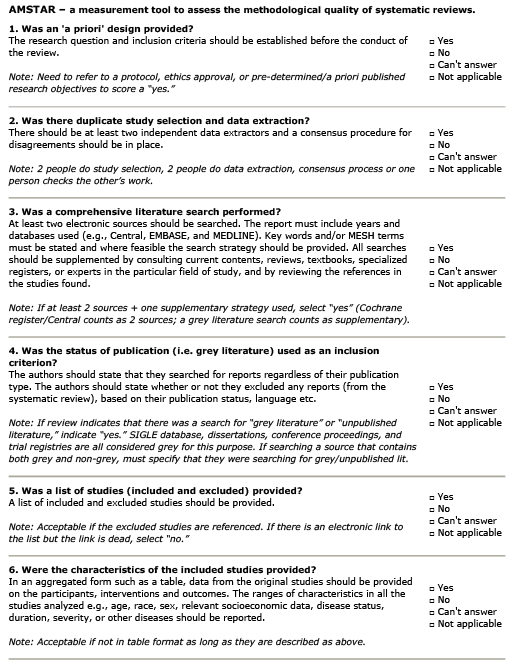
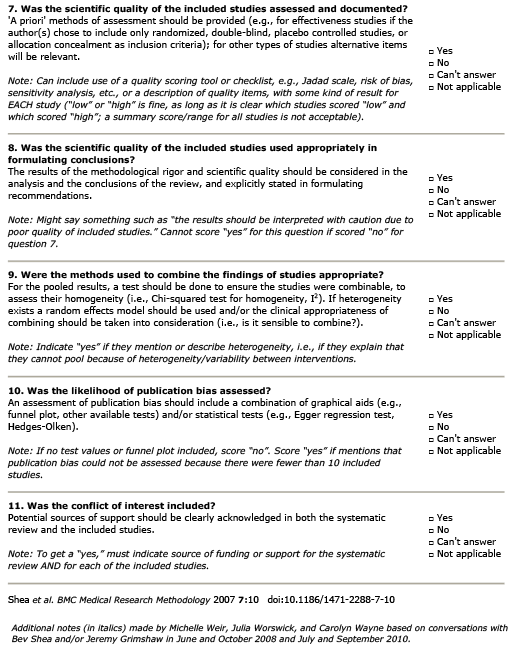
AMSTAR Rating
Summary
Patient Population:
14 randomized-control trials (RCTs) were included in this meta-analysis with a total of 862 participants presenting with chronic shoulder pain (at least three months of symptoms). The average age of the participants was 51 and diagnosis ranged between chronic shoulder pain, adhesive capsulitis (frozen shoulder), osteoarthritis, calcific tendinitis, subacromial impingement syndrome, and chronic subacromial bursitis.
Intervention:
The meta-analysis examined the implications of multiple interventions including corticosteroid injection (CSI), hyaluronic acid injection (HAI), suprascapular nerve block (SSNB), extracorporeal shock wave therapy (ESWT), kinesio taping (KT), and conventional physiotherapy program (CPT).
Comparison:
All studies included control groups that underwent CPT alone as treatment for their shoulder pain. This ranged in length of intervention from 4 to 12 weeks.
Outcome:
Various outcome measures were used to assess the pain and function of the interventions. The Visual Analog Scale (VAS) score, Shoulder Pain and Disability Index (SPADI) pain, SPADI disability, SPADI total, flexion range of motion (ROM), abduction ROM, and external rotation ROM were used throughout the studies.
– At 12 weeks, compared to CPT alone, intervention groups combining CPT and SSNB showed a statistically significant reduction in VAS score (MD: -0.56; 95% CI: -0.96 to -0.16; P < 0.05) and SPADI pain scores (MD: -12.60; 95% CI: -19.79 to -5.41; P < 0.05).
– Compared to CPT alone, intervention groups combining CPT and SSNB showed no statistically significant reduction in SPADI disability scores (MD: -8.32; 95% CI: -24.73 to 8.09; P > 0.05) and SPADI total scores (MD: -7.23; 95% CI: -17.80 to 3.33; P > 0.05).
– At 12 weeks, compared to CPT alone, intervention groups combining CPT and SSNB showed a statistically significant improvement in flexion ROM (MD: 15.20; 95% CI: 1.56 to 28.85; P < 0.05), abduction ROM (MD: 22.02; 95% CI: 4.70 to 39.35; P < 0.05), and external rotation ROM (MD: 16.48; 95% CI: 8.08 to 24.88; P < 0.05) with the highest probability (81.2%, 84.5%, and 93.5% respectively) of being the best intervention examined in the meta-analysis.
Guideline Recommendations
| Source | Recommendation |
|---|---|
| Journal of Orthopaedic & Sport Physical Therapy’ | Insufficient evidence to formulate a recommendation |
Outcomes Assessed
- Benefit
- Harm
- Inconclusive
SSNB and PT v PT alone
Pain @ 12 weeks
ROM @ 12 weeks
Function @ 12 weeks
Relevant Clinical Info
Mardani-Kivi M, Nabi BN, Mousavi MH, Shirangi A, Leili EK, Ghadim-Limudahi ZH. Role of suprascapular nerve block in idiopathic frozen shoulder treatment: a clinical trial survey. Clin Shoulder Elb. 2022 Jun;25(2):129-139. doi: 10.5397/cise.2021.00661. Epub 2022 May 16. PMID: 35698782; PMCID: PMC9185110.
Mardani-Kivi et al. (2022) was the largest RCT included in this meta-analysis, examining the impact of SSNB in patients with adhesive capsulitis (frozen shoulder). This non-blinded clinical trial included patients with stages 1 and 2 (based on Kisner and Colby’s classification system) adhesive capsulitis for at least three months. 97 participants (Male=40, Female=57, average age of 48.55) were split into three groups; physiotherapy (PT), intra-articular corticosteroid injection (IACI) + PT, and SSNB + PT group. All patients received Celecoxib 200 mg BID (twice a day). Both the IACI and SSNB group received a single injection of 8cc lidocaine HCL 1% and 2mL (80 mg) of methylprednisolone acetate- groups differentiated by approach (intra-articular versus suprascapular nerve injection). Over 12 weeks, the researchers found that the SSNB had a stronger recovery over all outcome measures compared to the PT and IACI groups. Abduction increased by 24.2° and 15.5° more in SSNB compared to PT and IACI respectively. Flexion increased by 21.1° and 8.3° more in SSNB compared to PT and IACI respectively. External rotation increased by 16.2° and 10.1° more in SSNB compared to PT and IACI respectively. Internal rotation increased by 12.7° and 6.3° more in SSNB compared to PT and IACI respectively. SPADI scores decreased by 10.34 and 7.57 points more in SSNB compared to PT and IACI respectively. VAS scores decreased by 0.6 and 0.4 points more in SSNB compared to PT and IACI respectively (for all measures P = 0.001).
Participant Information
The sample size was 862
Mean age of 51 years.
There were 14 studies used.