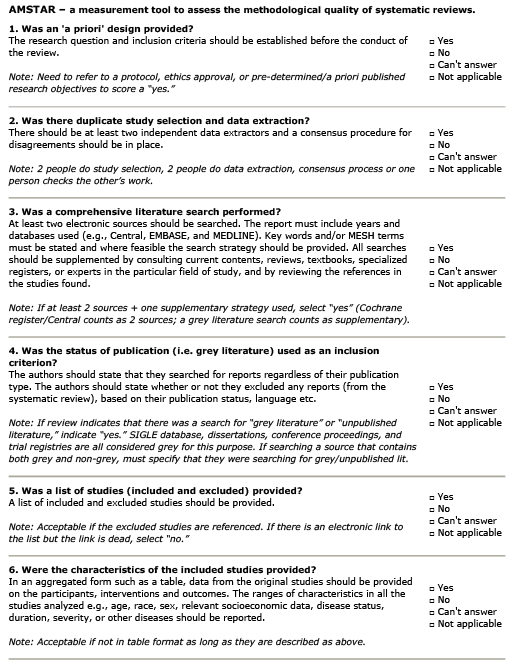
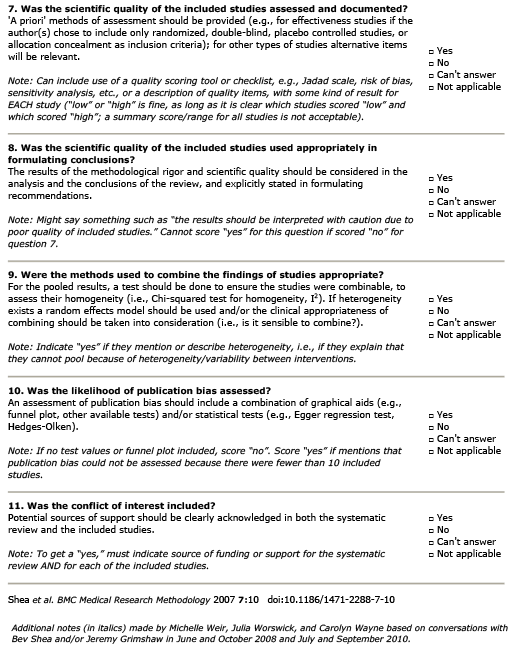
What is the evidence for trigger point injections for myofascial pain?
AMSTAR Rating
Summary
Patient Population:
15 RCT studies which involved a total of 599 patients with diagnoses including shoulder, back, head and neck pain, whiplash syndrome, craniofacial pain, cervicogenic headache, and osteoarthritis.
Heterogeneous data sets prevent combined meta-analysis.
Intervention:
Muscle based trigger point injection using a variety of substances including sterile water, saline, local anaesthetic and botulinum toxin.
Comparison:
Several comparisons including therapeutic ultrasound, laser treatment, stretching and dry-needling.
Outcome:
– Trigger point injection (TPI) (Water): Limited evidence that water TPI is more effective than saline TPI. No difference in safety between the two treatments. Follow-up = 8 months.
– TPI (Local Anaesthetic (LA)): Limited evidence that lidocaine TPI is more effective than sphenopalatine ganglion block. Follow-up = 1 week. Limited evidence that TPI (tropisetron) is more effective than TPI (LA) in relieving pain. No difference in safety between the two treatments. Follow-up = 8 weeks.
– TPI (LA) and Stretching: Limited evidence of no difference in effectiveness between TPI (LA) and laser or ultrasound. Combined TPI/neck stretching and ultrasound/neck stretching were more effective than neck stretching alone. TPI (LA) was more effective than dry needling. No difference in safety between TPI (LA) and laser. TPI (LA) caused less discomfort at injection than dry needling. Follow-up range = 4 weeks to 6 months.
– TPI (LA) and Dry needling: Limited evidence of no difference in effectiveness between the treatments. Safety outcomes not reported. Follow-up = 24 hours.
– TPI (LA) and intra-articular injection of Knee for OA: Limited evidence that TPI + intra-articular injection is more effective than intra-articular injection alone. No difference in safety between the two treatments. Follow-up = 21 days.
– TPI (Botulinum toxin): Moderate evidence of no difference in safety or effectiveness between botulinum toxin TPI and saline TPI, regardless of botulinum toxin concentration (50 U to over 200 U).Limited evidence of no difference in safety or effectiveness between 50 U and 100 U of botulinum toxin. Follow-up range = 16 weeks. Limited evidence of no difference in safety or effectiveness between the two treatments. Follow-up = 4 weeks.
– TPI (Botulinum toxin) and Physiotherapy: Limited evidence of no difference in safety or effectiveness compared to TPI (LA) treatment. Follow-up = 12 weeks. Limited evidence of no difference in safety or effectiveness between the two treatments, regardless of botulinum toxin concentration (10 U to over 50 U). Follow-up = 12 weeks.
– TPI (Botulinum toxin) and Stretching: Moderate evidence of no difference in safety or effectiveness between botulinum toxin TPI and TPI (LA), regardless of botulinum toxin concentration (10 U to 25 U). Limited evidence that botulinum toxin TPI is more effective and causes less discomfort than dry needling. Follow-up range = 4 to 10 weeks.
Outcomes Assessed
- Benefit
- Harm
- Inconclusive
TPI (Water) v. TPI (Saline)
Pain
TPI (LA) and stretching v. Stretching alone
Pain
TPI (Botulinum toxin) v. TPI (Saline or LA)
Pain
TPI (Botulinum toxin or LA) v. Dry needling
Pain from procedure
Participant Information
The sample size was 599
There were 15 studies used.