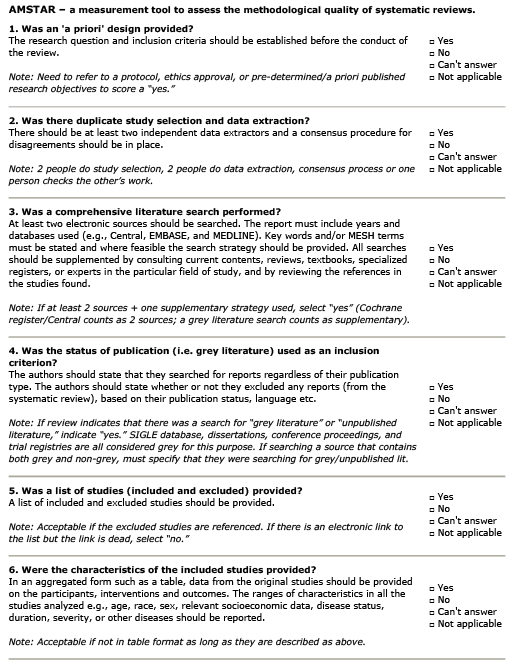
What is the evidence for physiotherapy interventions in the treatment of osteoarthritis of the knee?
AMSTAR Rating
Summary
Patient Population:
≥70% study participants were female. Recruitment was limited primarily to older adults with knee OA. Most were overweight – reported BMI averages 29 kg/m2. Approximately ½ of participants were prescribed concomitant anti-inflammatory medication or pain relievers in addition to PT intervention.
Intervention:
Interventions included: aerobic exercise, aquatic exercise, strengthening exercise, ultrasonography, proprioception exercise, T’ai Chi, education programs, diathermy, orthotics, magnetic stimulation.
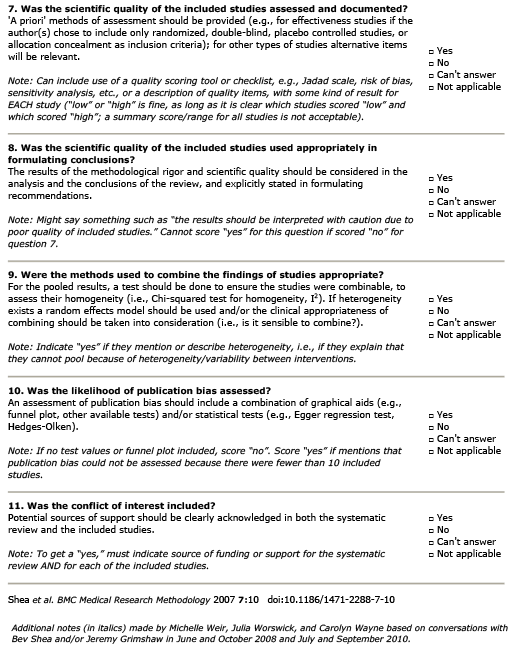
Comparison:
There were 212 articles identified (corresponding to 193 RCTs). Most RCTs demonstrated adequate randomization; however, concealment of allocation was unclear in the majority of trials identified (129/193). In addition, there was no planned ITT analysis described in 118 trials. One-third of the studies identified for inclusion did not describe masking of outcome assessment. 84 trials contributed data for pooling with regard to pain, physical function and disability. The strength of evidence was downgraded overall due to the risk for bias and low precision (wide CIs) associated with estimated treatment effects.
Outcome:
-
Education Interventions: Based on the pooled results from 2 RCTs, there is low-strength evidence that education programs had no effect on pain.
-
Pain: proprioception exercise vs. comparison not reported (4 RCTs) – significant difference in favour of exercise (SMD=-0.71; 95% CI -1.31 to -0.11).
-
Pain: aerobic exercise vs. comparison not reported (11 RCTs) – significant difference in favour of exercise at >26 weeks (SMD=-0.21; 95% CI -0.35 to -0.08).
-
Disability: aerobic exercise vs. comparison not reported (11 RCTs) – significant difference in favour of exercise at 3 months (SMD = -0.21; 95% CI, -0.37 to -0.04).
-
Function: aerobic exercise vs. comparison not reported (11 RCTs) – significant difference in favour of exercise at 3 months (SMD=-15.4; 95% CI -24.8 to -5.92).
-
Disability: aquatic exercise vs. comparison not reported (3 studies) – significant difference in favour of exercise (SMD=-0.28; 95% CI -0.51 to -0.05). There was no significant effect on pain or QOL.
-
Pain: strengthening exercise vs comparison not reported (9 RCTs) – significant difference in favour of exercise (SMD=0.68; 95% CI -1.23 to -0.14).
-
Function: strengthening exercise vs comparison not reported (9 RCTs) – significant difference in favour of exercise (SMD=-1.0; 95% CI, -1.95 to -0.05).
-
Strengthening exercise: strength of the evidence was rated as low due to risk of bias and the presence of heterogeneity (64%). Using meta-regression to explore heterogeneity demonstrated that, in terms of pain relief, younger participants experience significantly better outcome (p=0.02). Subgroup analysis (subset of studies) demonstrated that use of strengthening exercise was associated with long-term pain reduction (SMD=-12.8, 95% CI -22.9, -2.7).
-
Function: t’ai chi vs. comparison not reported (3 studies) – significant difference in favour of tai chi at 3 months (SMD = -0.44; 95% CI -0.88 to 0.00). There was no significant effect on pain or QOL.
-
Function: massage vs. comparison not reported (3 studies) – significant difference in favour of massage at 3 months (SMD = -0.55; 95% -0.93 to -0.18). There was no significant effect on pain or QOL.
-
Function: subtalar strapping vs. comparison not reported (7 studies) – significant difference in favour of subtalar strapping at 3 months (SMD=-0.27; 95% CI -0.53 to -0.02). There was no significant effect on pain or QOL.
-
Orthotics: No significant effect on function or pain.
-
Taping: No significant effect on function or pain.
-
Pain: electro-stimulation vs. comparison not reported (7 studies) – significant difference in favour of ES in the short-term (SMD=-0.71; 95% CI -0.98 to -0.43; VAS=15.6mm).
-
Pain: electro-stimulation vs. comparison not reported (7 studies) – electro-stimulation associated with an increase in pain at 6 months (SMD=0.57; 95% CI 0.09 to 1.06; VAS=12.5 mm).
-
Pulsed Electromagnetic Fields: No significant effect on function or pain (4 studies).
-
Pain: ultrasound vs. comparison not reported (6 RCTs) – significant difference in favour of ultrasound (SMD=-0.74; 95% CI -0.95 to -0.53; VAS = 16.3 mm).
-
Function: ultrasound vs. comparison not reported (6 RCTs) – significant difference in favour of ultrasound (SMD = -1.14; 95% CI -1.85 to -0.42; WOMAC change = 21.2 points).
-
Pain: diathermy vs. comparison not reported (5 studies) – significant difference in favour of diathermy in the short term (SMD=-0.53; 95% CI -0.96 to -0.1). No significant effect on function or gait.
Guideline Recommendations
| Source | Recommendation |
|---|---|
| ACR (2019) | Generally favourable but mixed recommendations (see guideline) |
| AAOS (2013) | Strong evidence for use |
Outcomes Assessed
- Benefit
- Harm
- Inconclusive
Educational Interventions
Pain
Proprioception Exercise
Pain
Aerobic Exercise
Pain
Disability
Function
Aquatic Exercise
Disability
Pain
Function
Strengthening Exercise
Pain
Function
T'ai Chi
Function
Pain
QOL
Massage
Function
Pain
QOL
Subtalar Strapping
Function
Pain
QOL
Orthotics
Pain
Function
Taping
Pain
Function
Elecrtostimulation
Pain @ 6 weeks
Pain @ 6 months
PEMF
Pain
Function
Ultrasound
Pain
Function
Diathermy
Pain
Function
Gait