What is the evidence for walking aids in the treatment of osteoarthritis of the knee?
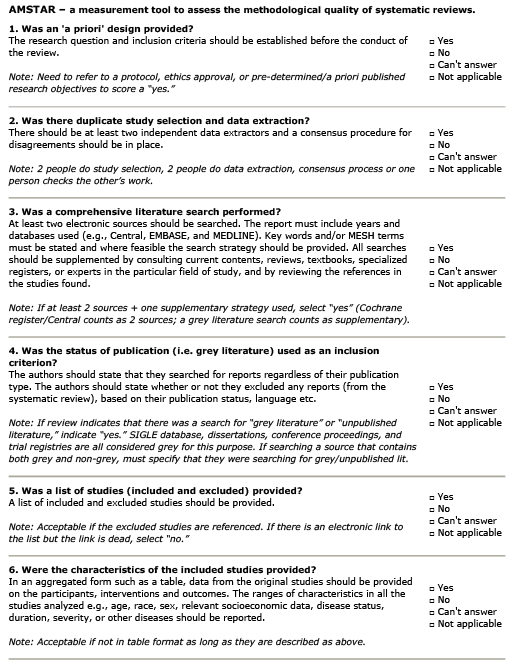
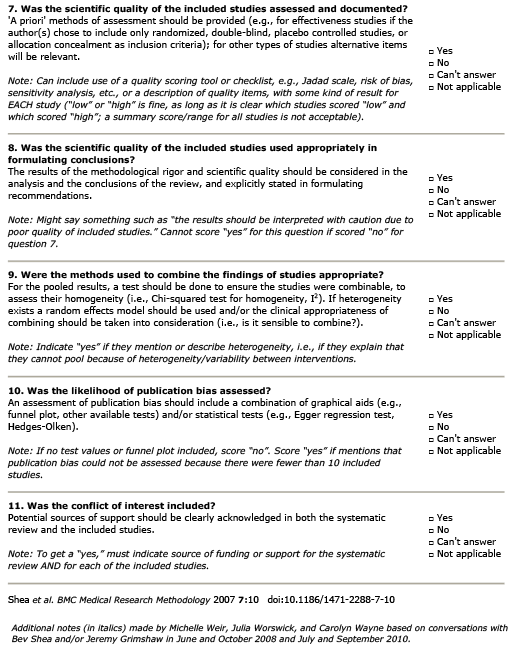
AMSTAR Rating
Summary
Patient Population:
14 studies included health participants only. 6 studies included only individuals knee OA. Individuals in the studies of knee OA tended to be older than the health adult studies. Mean ages reported in the OA studies ranged from approximately 58 – 67 years (with the exception of a case study – aged 37).
Intervention:
A variety of modifications were evaluated: inc./dec. toe-out (7 studies), inc./dec. gait speed (7 studies), contralateral cane use (2 studies), ipsilateral cane use (1 study) and Nordic walking poles (1 study). Knee thrust patterns appeared in 3 studies, increased step width in 2 (single subject design). Single studies examined weight transfer to the medial foot, increased knee flexion and reduced vertical acceleration at initial reduced stride length, increased medio-lateral trunk lean T’ai Chi Gait.
Comparison:
There were 24 studies identified that met all of the inclusion criteria for the present review. There were no RCTs identified – all studies used a within-subjects design and evaluated an immediate before and after effect of the intervention with the exception of 2 studies that included follow-up at 1 and 9 months. External knee adduction moment (KAM)(% change in early and late stance phases) was measured. Early stance peak was reported in 12 studies, late stance in 6. Early and “overall” stance were reported most frequently.
Outcome:
-
Increased toe-out: Changes in early-stance KAM ranged from a reduction of 55.2% to an increase of 12.9%; however, most of the changes demonstrated did not reach statistical significance. In late stance, there were reductions of 22.9% – 92.6% (with the exception of one study in which the baseline was 0.003 Nm/kg – p.412).
-
Reduced toe-out: There were small reductions in early-stance KAM (4.4 – 13.5%), although 1 study reported a 20% increase. Late-stance results were inconsistent.
-
Gait Speed: Increased gait speed in early stance was associated with increases in early stance KAM (up to 34.8%). There were small reductions in late stance KAM noted in healthy participants and participants with OA (8.3 – 12.9%). There were inconsistent results associated with reduced gait speed.
-
Cane Use: Contralateral cane use was associated with reduction in early-stance KAM (2 studies) (7.3-10.1%). There was also a reduction in late-stance (15.4%). However, ipsilateral cane use was associated with a 40% increase in early stance KAM.
-
Nordic Poles: Use of these aids was associated with an increase of early-stance KAM (14.8%) that was maintained through the late-stance.
-
Increased Step Width/Stride Length: Small reductions were noted in both early-stance (4.7-15.4%) and late-stance (9.5-11.7%) KAM. Reductions in stride length (without altering speed) did not change peak KAM, but was associated with small reductions in KAM impulse.
-
Knee thrust pattern(s): Medial knee thrust gait pattern resulted in reductions in KAM in both early (43.8% – 50%) and late phases (17%-55%). There was also a significant reduction in early KAM associated with internal hip rotation and adduction (20.9%).
-
Weight Transfer/Biofeedback devices: Combining the use of an “active biofeedback device” (p.412) (Note: in the table this is described only as the “shoe active feedback system”) with weight transfer toward the “medial foot” was associated with a reduction in early stance KAM (14.2%). Use of a knee biofeedback brace was associated with increased peak KAM (11.8%).
-
Tai Chi Gait: Use of this technique was associated with an increase in early-stance KAM (102.3%).
Guideline Recommendations
| Source | Recommendation |
|---|---|
| ACR (2019) | Strongly recommended |
Outcomes Assessed
- Benefit
- Harm
- Inconclusive
Contra lateral cane use
Knee adduction moment
Ipsilateral cane use
Knee adduction moment